We recently developed a project summary for an ESRC-funded study looking at the impact of the financial crisis and subsequent austerity measures on mental health and wellbeing in the UK. The summary for the CRESH project (full title: Recession, austerity and health: changing area socio-economic conditions and their relationship to individual health and wellbeing outcomes in Scotland) includes the key findings, links to papers published, details of some of the dissemination activities, and other useful resources. You can read more in the pdf below:
Category: wellbeing
-
What next for tobacco control in Scotland?
New research from the CRESH team using data from 124,566 shopping baskets purchased in convenience stores across Scotland has found that the purchase price of tobacco is lower in more disadvantaged neighbourhoods, largely because of the higher sales of the cheapest brands in these areas.
Cigarette smoking is one of the leading causes of preventable ill-health, hospitalisations and deaths in Scotland. Approximately 19% of adults in Scotland smoke, this rises to 32% in our most deprived fifth of neighbourhoods and falls to 9% in the most affluent neighbourhoods. As Scotland moves towards a ‘Tobacco Endgame’ the Scottish Government have a target to reduce smoking prevalence to less than 5% by 2034. A recent review of smoking projections by CRUK however suggests that Scotland may miss this target by 16 years in the poorest neighbourhoods. It is important that we continue to explore all potential determinants of smoking, particularly those that drive smoking in our most deprived communities.
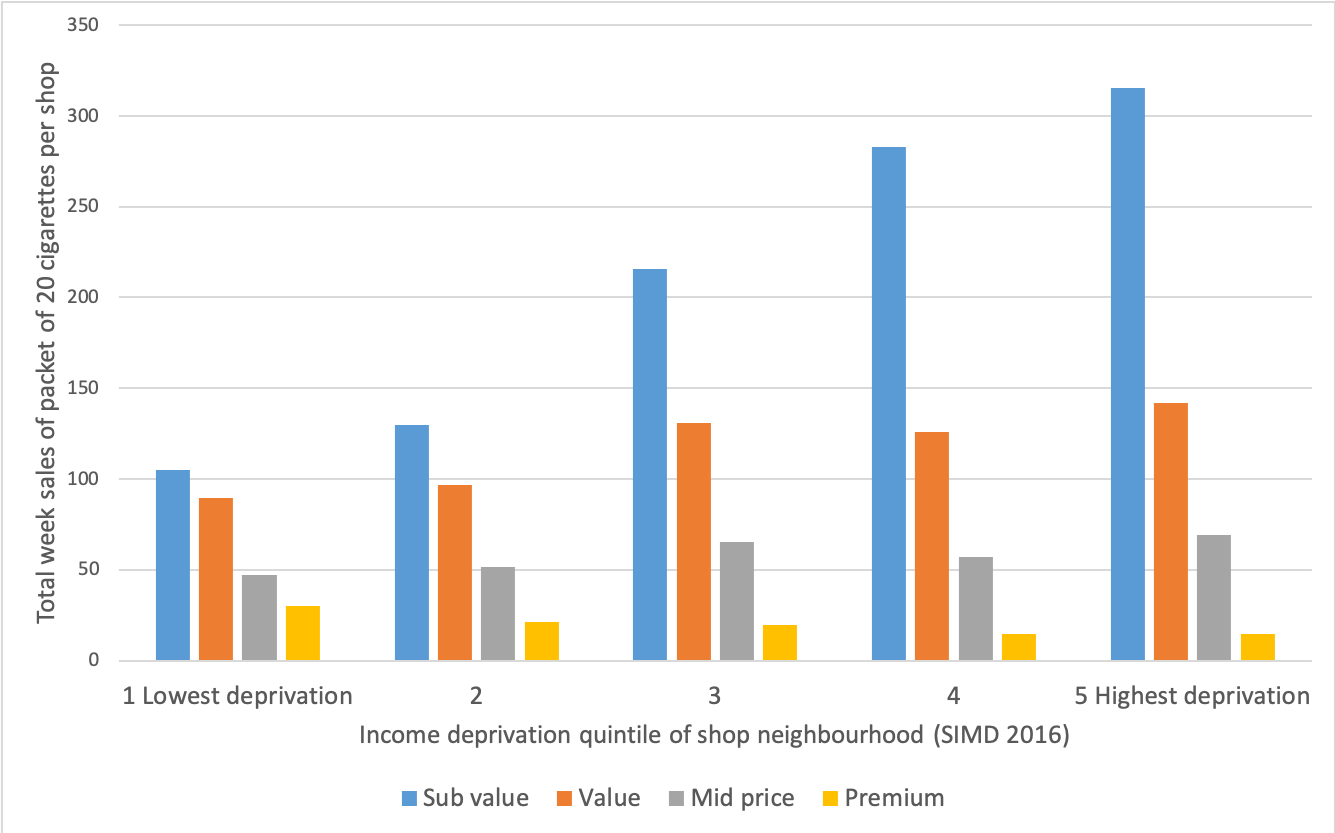
We know that tobacco price is one of the most important determinants of smoking behaviour and that many smokers are price sensitive. Whilst it may appear that all tobacco products are becoming increasingly expensive, research suggests that the average tobacco price in the UK has remained relatively unchanged in real terms over the past 20 years in spite of numerous tax increases. A practice, known as ‘undershifting’, has seen tobacco companies limit price increases on the cheapest brands and instead increase the price of the most expensive brands by larger margins, thus absorbing the tax increases on the cheapest cigarettes allowing them to remain cheap (Hiscock et al. 2018). As a result, the price of the lowest priced cigarette brands has remained relatively steady and the tobacco market as a whole has become increasingly stratified by price between the cheapest ‘sub value’ , ’value’, ‘mid price’ and high priced ‘premium’ brands. We wanted to understand these differentials in price a little better, so we carried out some research that was published recently in Tobacco Control. We explored whether the price paid for tobacco (both cigarettes and roll your own tobacco) was different in different types of neighbourhoods. We compared areas by deprivation, by the density of tobacco outlets and by rurality.
We analysed tobacco purchase data provided to us by The Retail Data Partnership. We looked at more than 124,000 purchases in 274 stores across Scotland in April 2018. For cigarettes the average price paid for a pack of 20 was £8.49, ranging from £7.20 to £13.25. For roll your own tobacco (RYO) 30g the average price paid was £12.14, with prices ranging from £9.80 to £15.99. We found that the price paid for tobacco did vary by neighbourhood type. In neighbourhoods with the lowest average household income the average purchase was 50p less for a pack of 20 cigarettes, and 34p less for roll your own tobacco compared with the most affluent neighbourhoods.
We then asked whether this was driven by individual brands being cheaper in more deprived areas, or whether cheaper, sub-value, brands were just more popular in such places. We found little evidence that individual brands were priced differently. Although the cheaper brands are the most popular in all neighbourhoods and across Scotland, accounting for 52% of sales, there’s a big difference in popularity between more and less deprived areas, In the most deprived areas these brands account for 58% of sales, but in most affluent areas it was just 39% (See Figure 1 below). So, it is the dominance of cheaper brands in more deprived areas that drives the 50p difference in average price paid per pack between deprived and affluent areas. Remember this matters because the tobacco companies work to subdue tax-based price rises on the cheapest brands.
We also explored whether the density of tobacco retailers and/or rurality had an impact on tobacco price. We found little evidence of a density effect, but we did find that the individual brands analysed were significantly cheaper in rural areas.
So what does this mean and what can we take from this research? It is clear from the CRUK review that we need to work harder in order to reach the 2034 target of less than 5% of the population smoking. Price is a lever that we can pull, but to date this has been largely done through tax increases. This research shows us that the cheapest brands are the most popular in all neighbourhood types, but much more so in our most deprived neighbourhoods where smoking rates are highest. We found that the price paid for tobacco is lower in more deprived areas compared to more affluent areas. Our results confirm that the dominance of cheaper, so called ‘sub-value’ brands in more deprived areas, is a driving force behind the difference in price paid for tobacco between neighbourhoods. This highlights the importance of cheaper tobacco products to the consumer and the market. Cheap tobacco may help tobacco companies to retain price sensitive consumers who live in the most deprived areas, which, in turn, contributes to health inequalities. In addition to increases to the duty rates on tobacco, more radical policy responses are likely to be required. These include a combination of minimum unit pricing (MUP) and a price cap at the upper end. The MUP would raise the cost of cheaper cigarettes and the price cap at the upper end would prevent the more expensive brands being used to ‘protect’ the cheaper ones from tax rises.
With growing international interest in the ‘Tobacco Endgame’, policymakers should identify measures that counter industry tactics that enable the continued sales of cheap tobacco. We published this paper in the first week of the COVID-19 pandemic in the UK. These are clearly strange times and we should rightly focus on the public health impacts of the global pandemic, and in particular the vast health inequalities that are arising. We must not however forget that the public health challenges we were faced with before this pandemic remain. Tobacco, and other unhealthy commodities, require our attention and the inequalities that arise from them remain a matter of social justice.
You can find the paper here:
References
Hiscock R, Branston JR, McNeill A, et al. Tobacco industry strategies undermine government tax policy: evidence from commercial data. Tob Control 2018;27:488 LP – 497. doi:10.1136/tobaccocontrol-2017-053891
-
New ESRC funded study on Tobacco and Alcohol
We are delighted to announce that we have been awarded funding from the ESRC for a project exploring tobacco and alcohol environments in Scotland. The project ‘Change in alcohol and tobacco availability, population health and the lived experience’ will be funded for 3 years, beginning December 2019 for a total of £761, 470. The project will be led by Professor Niamh Shortt with co-investigators from the University of Edinburgh (Professor Jamie Pearceand Dr Tom Clemens), Glasgow Caledonian University (Professor Carol Emslie) and the MRC/CSO Social and Public Health Sciences Unit, University of Glasgow (Professor Richard Mitchell).
This research will measure change in the availability of alcohol and tobacco in Scottish neighbourhoods over time and explore how this change relates to health outcomes and how residents experience the availability of alcohol and tobacco in their neighbourhoods. The findings will be important because smoking and alcohol consumption are leading causes of illness and death. In Scotland smoking causes one in every 5 deaths and one in 20 deaths is related to alcohol. This harm is not equally shared; those on the lowest incomes suffer the greatest harm. These illnesses and deaths are preventable. The World Health Organisation recommends that nations prioritise interventions that reduce the supply of alcohol and tobacco.
Why might neighbourhood supply of alcohol and tobacco matter? Research suggests that when there are a lot of outlets in a neighbourhood this impacts upon consumption in three ways. 1. The outlets may be more competitive and drive prices down to attract customers. 2. Oversupply may normalise the products when they are sold alongside everyday commodities, such as bread and milk. 3. Tobacco and alcohol may simply be easier to buy in areas where there are more outlets.
In order to explore the relationship between supply, behaviour and harm we need data on the location of every outlet in Scotland selling tobacco and/or alcohol. Ideally, to be able to say something about whether the relationship may be causal, we need this data over time. We have already collected data on the specific location of every outlet selling tobacco and licensed to sell alcohol over multiple time periods (2012 and 2016 (nationwide alcohol and tobacco – see paper here) and 2008 (alcohol in four cities – see paper here)). As part of this project we will collect updated data for 2019/20. This will allow us to measure this change over time. Using an approach called trajectory modelling we will group neighbourhoods that have had a similar degree of change; some neighbourhoods may have lost, or gained, local shops or pubs, whereas some may not have changed at all. We will then identify features of these neighbourhoods that may be driving this change, for example the age profile of the population or poverty levels. This will help policy makers understand the drivers of change in our neighbourhoods.
To measure the relationship between changing supply and harm we will link these trajectories, and our measures of availability at each time point, to alcohol and tobacco health outcomes (behaviour, illness and death). We will use statistical models to see whether areas experiencing an increase or decrease in outlets have seen a corresponding increase or decrease in these outcomes. This will allow us to get a better understanding of whether an over supply of alcohol and tobacco is related to smoking and alcohol consumption and harm. These findings will provide important evidence related to the provision of such commodities in our neighbourhoods.
Although these statistics are important to report we also need to understand why an oversupply of alcohol and tobacco may influence behaviour and harm. Whilst the literature suggests the pathways listed above, we know little about the experiences of individuals living in neighbourhoods with contrasting availability. We don’t understand the individual experience of any of these pathways. Professor Carol Emslie will lead a qualitative work package and researchrs will meet with groups of individuals, in neighbourhoods of contrasting trajectories, to talk to them about the supply of alcohol and tobacco. We will explore their experiences of neighbourhood and assess how their perceived notions of their neighbourhood availability contrast with our statistical measures. Finally, we will meet with residents, retailers and policy stake-holders to explore potential interventions related to supply. Policies at this level require public, retailer and political support. We will discuss the priorities held by various groups, present our quantitative results and gauge attitudes towards potential interventions.
Throughout the project will be committed to knowledge exchange, public events and speaking with non academic partners. If you wish to know more about this research, or would like one of the researchers to come to your organisation to provide you initial findings (once the project is under way) then contact the Principal Investigator here: niamh.shortt@ed.ac.uk
-

Mental health problems are common among prisoners in low-income and middle-income countries
In a major international review, we found very high rates of psychiatric and substance use disorders among prisoners in low-income and middle-income countries. The results from the systematic review and meta-analysis published in Lancet Global Health showed that the prevalence of psychosis, depression, and drug and alcohol use disorders is much higher in this marginalised population in comparison to the community, pointing to unmet needs and calling for action in research and policy.
Mental health and substance use problems are common among individuals involved in the criminal justice system. Incarcerated men and women often come from disadvantaged socioeconomic and family background, and frequently have a life history of victimisation and substance use, making them more vulnerable to mental health problems. While in prison, they often remain undiagnosed and untreated. Prisoners with unmet mental health needs have higher mortality, especially by suicide, and greater risk of recidivism and reoffending after release in the community, leading to multiple imprisonments.
Although 70% of the worldwide prison population are residing in low-income and middle-income countries (LMIC), almost all scientific evidence is coming from studies conducted in high-income countries. It is an important limitation as recommendations from a mostly Western context might not be applicable or generalizable to poorly resourced settings. Prison conditions in LMICs are usually very harsh, characterised by overcrowding, poor nutrition, and sanitation, and limited or complete lack of access to basic health care. To provide evidence for future research and policy making, we conducted a systematic review and meta-analysis on prison prevalence studies in LMICs.
After screening 6000 titles and abstracts from 17 electronic global databases, we identified 23 relevant publications based on 14,527 prisoners from 13 different LMICs. Considering a one year time interval, approximately 6.2% of the prisoners had psychosis, 16.0% major depression, 3.8% alcohol use disorders, and 5.1% drug use disorders. To illustrate the immense burden of mental health problems, we quantified the difference between the prevalence among prisoners in each sample and in the sex-matched general populations of the respective countries. Prevalence rates among prisoners were 16 times higher for psychosis, 6 times higher for major depression and illicit drug use disorder prevalence, and twice as high for alcohol use disorders, indicating a significant public health concern and large unmet health care needs in this marginalised group. Moreover, rates in prison populations of LMICs might be even higher than in high-income countries.
Based on our findings, we presented several implications and recommendations for research and policy.
- While a review from 2012 on prison mental health in high-income countries identified over 100 samples, we were able to find only 23 studies from a much larger and diverse group of countries. There is a need further evidence from LMICs to adequately plan interventions for prisoners with mental disorders, especially from regions underrepresented in research such as Central and East Asia, and Central America.
- Because correctional facilities in LMICs often lack basic health care, the implementation of cost-effective interventions and scalable treatments for individuals with mental health problems is crucial.
- Imprisonment could present an opportunity to treat people with mental health and substance use problems who otherwise would be difficult to reach for health services. National governments in LMICs should move the responsibility for prison health care from prison administrations to the national health services.
- Since human right violations, and physical and psychological abuse are more common in resource-poor correctional settings, increasing mental health literacy among staff and protecting the rights and health of people with mental illnesses should be a priority for penal justice policies.
The invited comment on our paper gives a valuable and very practical recommendation on how to improve mental health services in correctional facilities. Training prison health workers by mental health professionals using the WHO’s Intervention Guide for mental disorders (mhGAP-IG), could be a cost-effective and valuable programme for addressing the treatment gap among prisoners in LMICs and coming closer to the Sustainable Development Goals declared by the United Nations.
By Gergo Baranyi, PhD Student in Human Geography and Marie Sklodowska-Curie Early Stage Researcher, The University of Edinburgh
-
What is ‘on the ground’ in a city linked to levels of inequality in life satisfaction
In a European-wide study of 63,554 people from 66 cities in 28 countries, we found links between urban design and levels of inequality in life satisfaction. This is the first study to theorise and examine how the entire urban landscape may affect levels of and inequalities in wellbeing in a large international sample.
Cities with an even distribution of facilities, housing and green space were linked with lower levels of inequality between residents’ life satisfaction levels, suggesting that more equal access to a range of facilities and types of land may help reduce the gap in life satisfaction between the most economically-deprived and most affluent residents of a city.
There was a strong link between higher life satisfaction and living in cities with homes surrounded by natural, green space. However, lower life satisfaction was linked to living in cities that had more wasteland, more space dedicated to housing, and more space in which all the land is concrete or tarmacked.
Implications for policy and planning.
The findings of our study suggest that urban planning has a role to play in addressing inequalities in cities. Our finding that more equal distribution of land cover/use is associated with lower levels of socio-economic inequality in life satisfaction supports the idea that city environments could be equigenic – that is, could create equality.
What people want or need from their city varies moment to moment, day to day, life stage to life stage. If a city is varied enough to offer people what they need, when they need it, it is likely to support a higher quality of life.

Why understanding city design is important for population health and well-being?
With the United Nations reporting that more than half the world’s population residing in urban areas and this proportion rising, it is important to understand how well-planned urban environment might improve, and reduce inequalities in, quality of life. Therefore, understanding the influence urban environments can have on all aspects of health and wellbeing is increasingly important. Cities are continuously evolving and there is ample opportunity to ensure these are healthier and happier place to live.
What we did:
We applied theory and methods from landscape ecology to explore associations between cities’ land cover/use, residents’ reported life satisfaction and within-city socio-economic inequalities in life satisfaction. We joined individual-level responses to the European Urban Audit (EUA) Perception Surveys (2012 and 2015) with city-level data from the European Urban Atlas classifying land cover/use into 26 different classes. Our sample included 63,554 people from 66 cities in 28 countries.
The study, ‘Are urban landscapes associated with reported life satisfaction and inequalities in life satisfaction at the city level? A cross-sectional study of 66 European Cities’ is published in Social Science & Medicine (Open Access). The work was funded by The Medical Research Council (MRC) and Scottish Government Chief Scientist Office.
By Rich Mitchell, Natalie Nicholls & Jon Olsen , Neighbourhoods and Communities programme, MRC/CSO Social and Public Health Sciences Unit, University of Glasgow.
-
Changing places and mental health: do changes in perceptions of neighbourhood influence anxiety and depression in adults?
Written by Dr Jon Olsen, Research Associate with the Neighbourhoods and Communities programme, MRC/CSO Social and Public Health Sciences Unit. This blog is mirrored on the SPHSU website.
Mental health problems are a global issue. In 2013 over 615 million individuals suffered from anxiety and/or depression across the world, a rise of 50% since 1990. How people experience their local environment can impact on mental health. Living in areas that are perceived to have higher levels of neighbourhood problems such as poor housing quality, limited amounts of greenspace, industrial activity, and high traffic volume, has been linked to poorer mental health by some research studies. But, few studies have explored how change in what people think about their neighbourhood is linked to change in their mental health. It would be useful to know this as improving the neighbourhood environment could strengthen mental health.
In our recently published study, we wanted to see how changes in what people thought about their neighbourhood impacted on residents’ mental health over time. We looked at two mental health outcomes: anxiety and depression. Adults who lived in West Central Scotland, an area including Glasgow and eight neighbouring local authorities, were asked to complete the same questionnaire in 1997 and 2010.

Glasgow, United Kingdom – October 20, 2013: People come to walk around and shop at the historic Barras Market Place flea market. What did we find?
Overall, anxiety and depression in the people we spoke to reduced between 1997 and 2010. However, those who experienced worsening neighbourhood perceptions from 1997 to 2010 also had increased anxiety and depression scores.
Why this matters
Our study showed that worsening neighbourhood perceptions were linked with small increases in anxiety and depression scores. People living in areas where perceptions of the neighbourhood got worse, did not benefit from the general improvements in anxiety and depression scores enjoyed by the population as a whole; this could widen health inequalities.

Wheelie bins (blue for recycling, green for general refuse) lined up for collection in a Glasgow alley. The take home message from this study
There is a clear need for national and local policy to target areas where neighbourhood conditions are substantially deteriorating to ensure people’s mental health does not suffer.
Further information about the study
We used data from the Transport, Housing and Well-being study; a postal survey of adults in eight local authority areas in the west of Scotland in 1997 and 2010. More information and a link to the full questionnaire can be found here: http://thaw.sphsu.mrc.ac.uk/.
Anxiety and depression was measured using the Hospital Anxiety and Depression Scale (HADS), a common measure of psychological distress that has been in use for over 30 years.
The full paper was published in the International Journal of Environmental Research and Public Health and is freely available here.
Disclaimer: The views expressed in this blog are those of the author.
The MRC/CSO Social and Public Health Sciences Unit is funded by the Medical Research Council and the Scottish Government Chief Scientist Office. The views expressed are not necessarily those of the Medical Research Council or the Scottish Government.
-

Edinburgh Science Festival Event 2017: Why Places Matter for Mental Health and Wellbeing
The important influence of the places in which we live, work and play on our mental health and wellbeing was the topic of a recent lively discussion at the Edinburgh Science Festival 2017 organized through Centre for Research on Environment, Society and Health (CRESH).
The event was chaired by Professor Jamie Pearce, (from School of GeoSciences at the University of Edinburgh and CRESH) and, in his introduction, he emphasised the policy-relevance of the event as evidenced by the Scottish Government’s newly released Mental Health Strategy 2017-2027. The Strategy details how institutions, services and organisations will work together to enhance mental health in Scotland. Especially relevant for this discussion was the acknowledgement on P8 of the report that ‘Working to improve mental health care is not just the preserve of the NHS or the health portfolio. We will be working not only across the Scottish Government, but also across the wider public services to harness the broadest range of opportunities to improve the population’s mental health…’. It is therefore acknowledged that promoting good mental health and wellbeing is not only about medical care, but also involves action to improve the ‘wider determinants’ of mental health – especially how conditions in the places where we live, work, learn and play can affect mental health and wellbeing.
We were therefore interested to explore how academic research contributes to our understanding of how places affect wellbeing. Our main aim was to exchange ideas with our audience of over 70 people, representing a range of views from those living in the communities in and around Edinburgh. Several participants also reported on knowledge and experience gained in their professional lives, including medical practitioners, public health specialists, leaders in independent organisations whose mission relates to mental health and wellbeing (such as Support in Mind, and the Cyrenians), urban planners and architects and social service providers.
The event started with a series of comments from a panel of academic researchers representing a variety of social science disciplines, who introduced ideas from academic research that may help to frame thinking on these issues.
Professor Sarah Curtis (Professor Emeritus at Durham University) used her own experience of volunteering in the Edible Garden project at the Botanic Gardens to illustrate ideas from Health Geography about Therapeutic Landscapes, originally put forward by Wil Gesler (e.g. in his book on Healing Places). This conceptual framework suggests we can think of places in terms of: material and physical landscapes (agreeable and relaxing green spaces, water spaces and built environments), social landscapes (supportive social relationships and community processes) and symbolic landscapes (features of our environment that stand for beliefs, principles and memories that are important for us). All of these dimensions of places, experienced in the different settings where we spend our lives, can be important for creating and maintaining our sense of mental wellbeing. These features of landscapes, the ways they change, and how different groups of people experience them over time, have been studied extensively by health geographers (e.g. reviewed by Sarah Curtis in her book Space, Place and Mental Health).
Professor Steve Platt (Professor Emeritus at University of Edinburgh) then presented ideas from research in Sociology and Health Policy about what we might consider the ‘reverse’ of therapeutic landscapes; focussing on factors that are associated with risk of suicide and why suicide matters for suicide prevention. He used the example of the iconic Golden Gate Bridge in San Francisco, which has been a ‘magnet’ for people intent on taking their own lives. He described the public controversies surrounding action to alter the architectural form of the bridge in order to install protective structures to reduce the suicide risk. He also underlined the evidence for socio-economic deprivation as a risk factor for suicide, with the risk of suicide being 2-3 times higher in the local areas in Scotland ranked among the worst 10% for social deprivation, as compared with populations living in areas ranked in the least deprived areas. He went on to elaborate further on the idea of suicidogenic contexts combining various dimensions that may be cultural, socio-economic, political, historical, as well as including built infrastructures and other aspects of the physical environment.
The significance for wellbeing of green space, viewed from a Landscape Architecture perspective, was introduced by Professor Catharine Ward Thompson, Director of the OPENspace Centre at the University of Edinburgh’s College of Art. She underlined that, since stress is a major problem for society and is associated with physiological as well as mental illness, researchers at OPENspace, together with their colleagues from around the world, are exploring how attractive and accessible green spaces can have beneficial ‘restorative’ effects on our mental state and help us to cope better with stress. Studies using biomarkers (that measure the functioning of psychoneuroendochrine systems in the human body) show that our mental and physical states are linked, which helps to explain why environments that help to restore mental wellbeing are also helpful for our physical health. Good access to green and natural spaces in the residential environment is associated with lower levels of stress as shown by these biomarkers, as well as from self-reports of stress among people out of work and living in urban poverty. Attractive green spaces are often also places where we enjoy supportive social relationships and healthy physical exercise. Conversely, when there is a shortage of green space in the urban environment, this appears to be associated with feelings of loneliness and lack of social support. Professor Ward Thompson has published research exploring these relationships in the journal Landscape and Urban Planning and the International Journal of Environmental Research and Public Health. Findings such as these help to strengthen the case for providing and maintaining access to healthy green spaces, such as public parks and gardens, allotments, and public rights of way in the countryside.
Dr Niamh Shortt (School of GeoSciences at the University of Edinburgh) leads research at CRESH relating to how aspects of consumption and retail environments are significant for behaviours linked to mental health and wellbeing. She focused her talk especially on issues associated with alcohol consumption and unhealthy drinking, which can be closely linked to mental distress and mental health conditions. While lower income groups report consuming the same, or less, alcohol on average than higher income groups, they suffer more from alcohol related harm. This has been called the ‘Alcohol Harm Paradox’. Dr Shortt presented findings from research she is leading which show that risks of unhealthy alcohol use are not only associated with individual level characteristics, but can also be influenced by the social and commercial environment. Access to and advertising of retail outlets selling alcohol is not currently controlled to the same extent as for tobacco sales, yet research is showing that there the ways people drink may be influenced by the organization and availability of alcohol retailing in their neighbourhood, and that this is especially important for those living in poorer areas who may be most reliant on their local retail facilities. This research demonstrates the importance for wellbeing of work of retail planning and licensing systems.
As the discussion widened to include the audience at this event, a number of other thoughtful and important points were made. We heard from a number of representatives of relevant non-academic organizations, explaining how actions to promote mental wellbeing and to prevent and treat mental illness may draw upon research, and also contributes to knowledge about ‘what works’ to promote wellbeing.
Dr Margaret Douglas, Consultant in Public Health Medicine for NHS Lothian, underlined concerns about the unequal impacts of places on both health for different groups in Scottish society. She highlighted links between physical and mental health. The geographical variations in mental health and wellbeing, and inequalities between rich and poor areas, are a major issue for public health in Scotland, as in other countries, so research is important to help to identify the places where health disadvantage is most concentrated and needs for mental health care are greatest. This said, not all of the people most at risk of poor mental wellbeing and mental illness live in the poorest areas, so that there is also a need for information on the social and geographical pattern of mental health problems across the whole of Scotland. Dr Douglas particularly noted the range of aspects of the environment that are important for health. Her comments drew attention to the range of partners who need to collaborate to address actions to improve the various environmental factors that are beneficial for wellbeing and can help to prevent mental health problems. The Scottish Health and Inequalities Impact Assessment Network has produced documents summarising evidence on several aspects of the environment including community venues, greenspace, transport and housing.
These comments were reinforced by Johnny Cadell, from Architecture and Design Scotland, who underlined the significance of Scottish Government architecture policy (Creating Places), Scottish Planning Policy and the Place Standard, which promote healthy environments across Scotland. The Place Standard is a joint initiative between Scottish Government, Health Scotland and Architecture & Design Scotland. The discussion highlighted the strong interest in how good urban design can benefit mental health. We noted that there is very good potential for the transfer of knowledge from research into policy and practice, and this is gaining momentum through collaboration between researchers and government agencies promoting various initiatives, such as work by the Design Council entitled ‘Active by Design’ and, in Scotland, initiatives such as ‘Good Places Better Health’, ‘Go Well in Glasgow’ and, most recently, the development of the ‘Place Standard Tool’ to guide local development. Increasingly, Health Impact Assessment is being applied to interventions outside the medical sector, to ensure that health impacts of new urban developments are considered at the planning stage. The Place Standard brings together commitments in architecture policy (Creating Places) to produce a tool linking spatial design with the health/wellbeing agenda and the commitment in Good Places Better Health to produce a ‘Neighbourhood Quality Standard’. Those involved in Good Places Better Health and Go Well were closely involved in the design of the new tool.
Frances Simpson, from Support in Mind, helpfully drew attention to the fact that a good deal of research is currently focussed on more urban communities, but that it is also important to understand the experience of the rural communities in Scotland. Among a range of activities promoted by Support in Mind is a project that is currently collecting valuable information on what it is like living with mental ill-health in rural Scotland. Communities in rural areas may benefit from greater proximity to extensive green spaces than those living in cities, but there are other issues such as social isolation and exclusion, and problems of access to the right kinds of mental health services, which need to be considered in rural settings. These points resonate with an article recently published by Hester Parr and Chris Philo in The Geographer magazine reporting research involving participants in rural areas.
Hugo Whitaker, from the charitable organization Cyrenians, also pointed out that recovering from mental illness can be a long process and that access to supportive environments over time can be very helpful to restoring mental wellbeing. He provided examples (including 2 film clips) of how community gardens and healthy activities organised in grounds that are part of NHS estates can help to restore and maintain good health.
A number of useful film clips have also been published by the Green Exercise Partnership to help spread the word about this kind of activity (see example film here), as well as recordings of individual accounts from the perspective of those involved in design and planning (here) and stories of patient users’ experiences: (here).
Also relevant to this debate is the Our Natural Health Service action programme. It shows how “high quality local greenspace, supportive nature-based projects, and better links between health and social care practitioners and the environment sector, can be part of the solution to many of Scotland’s health issues.” NHS Lothians’s report ‘Health Promoting Health Service: Action in Secondary Care Settings’ issued by the Chief Medical Officer in October 2015 includes targets on “current use and improved plans of the outdoor estate for physical activity (green exercise and active travel) for staff, patients and the local community” as well as targets for staff health and wellbeing.
The debate included further comments from a number of other members of the audience. Points made by the panel about long term effects were picked up on by a retired General Practitioner who practised in one of the most deprived areas in Scotland. He commented that deprivation was transmitted across generations and that the conditions causing mental health problems in one generation would resurface in the next generation who were also treated in his surgery. Research reporting on the environmental experiences of people at different life stages was considered. For example, experiences of adolescents were commented on and it was pointed out that mental health problems can become apparent relatively early in life, and that young people have relatively little control over the social and physical environment, so it is important for their voices to be heard in environmental planning processes. Aspects of the environment that are beneficial for wellbeing of young people vary from those which are important for adults, so their experience needs to be taken into consideration.
Individuals with different characteristics may react quite variably a given environment and research can help to improve understanding of how places interacting with personal characteristics relate to mental wellbeing. It was noted, for example, that people vary in terms of cognitive and physical abilities and that making public spaces well adapted and inclusive for people with a range of abilities can help to promote mental wellbeing for all ability groups.
Other comments underlined the importance of a sense of autonomy and freedom to exercise independence and choice in the way we interact with our environment. It was noted that it was not only the visual aspect of the environment that was important, and that it was important for architects and others designing the environment to be sensitive to aspects such as noise levels and ambient temperature which can also affect one’s sense of wellbeing in a particular setting.
Overall, this event clearly demonstrated the breadth of interest in the question of why places matter for mental health and wellbeing. The panel were very grateful to the audience for engaging in the discussion and making such thoughtful comments and to SciFest for organizing the event. We felt this was a good example of how academic researchers and others with relevant ideas and experiences can join together to ‘co-produce’ our understanding of the research agenda and how research can help to inform action. We hope to be able to keep in touch with participants, via the CRESH webpages and blog, in order to share future research findings and knowledge of what is important for our wellbeing in the places where we live.