
For most of my academic career, I have wrestled with a dilemma that I suspect many urban health researchers recognise, even if we do not always say it openly.
If the causes of health inequalities are structural, should we focus mainly on advocating for structural change? Or should we concentrate on practical interventions that might improve people’s lives right now, even if they do not transform the wider system?
Cities make this dilemma impossible to ignore. Walk across Glasgow, London or Bristol and you can cross more than a decade of life expectancy within a few miles. These inequalities are written into urban landscapes through housing, transport, employment, environmental quality and access to resources.
Early in my career, I worked mainly on documenting and explaining those structural inequalities. For example, we mapped health inequalities across Britain (see the example below) and modelled the potential effects of reducing child poverty or improving employment.
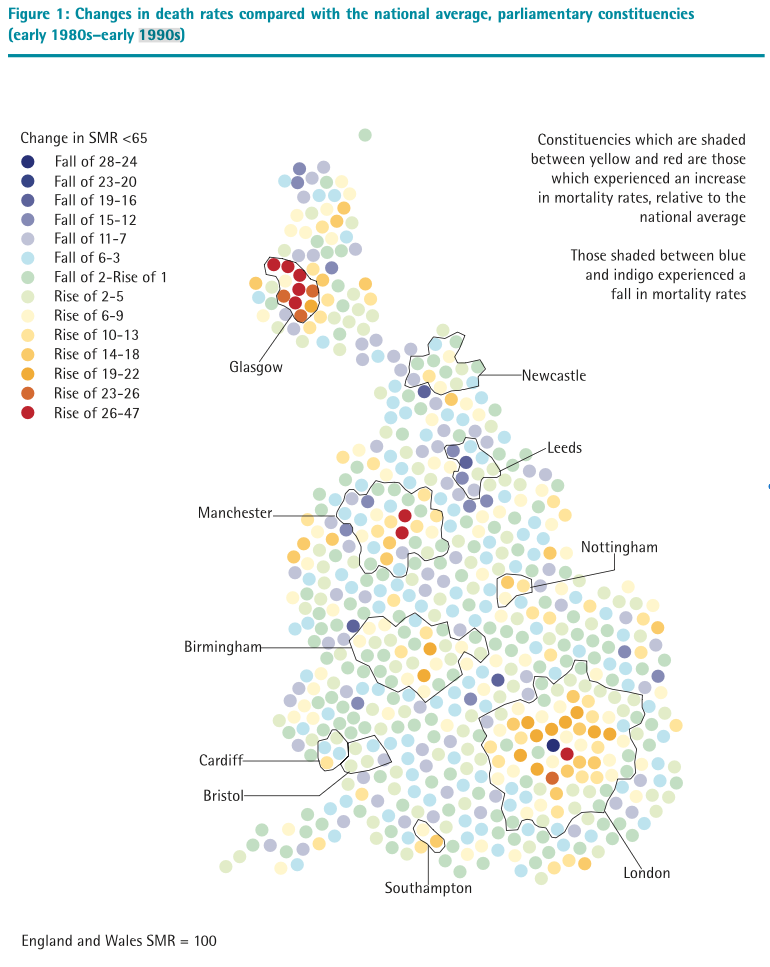
The logic was straightforward: if the causes of health inequality are structural, then the solutions must be structural too.
There is strong evidence for this position. Research on the “fundamental causes” of disease argues that inequalities in wealth, power and opportunity continually generate new pathways to poor health, even as older ones are removed. Urban geography similarly shows how cities reproduce inequalities spatially across generations through housing systems, uneven investment and segregated opportunity structures. In one article, we showed just how little the geographies of health and inequality had changed in London over a whole century.
Yet, over time I became increasingly frustrated. There was so much evidence pointing to large-scale societal change as the solution, but meaningful reform seemed politically distant. Meanwhile, whilst we advocated for those changes the inequalities persisted.
I also became uneasy with a tendency within parts of the field to dismiss smaller-scale interventions as distractions from the “real” structural causes of inequality. People living with poor health and disadvantage now cannot wait decades for ideal political conditions.
That tension gradually pushed my research in a different direction. I became interested in whether aspects of urban environments might help people stay healthier despite adversity. In particular, I began studying green space and health.
Over the past two decades, evidence has consistently shown that greener urban environments are associated with better mental and physical health. Some studies also suggest these benefits may be strongest for people living in more deprived circumstances. I later described such places as “equigenic” environments because they may help weaken the link between social disadvantage and poor health.
Of course, parks and trees are not substitutes for fair wages, good housing or well-funded public services. Neighbourhood improvements can also create new problems, including gentrification and displacement. Yet local environmental improvements can still make cities healthier and more liveable while broader structural changes remain contested or slow to emerge.
Increasingly, I think urban health research sometimes frames the issue wrongly. Structural reform and neighbourhood intervention are often treated as competing approaches when cities actually operate across multiple interacting scales at once. Housing, transport, planning, labour markets and neighbourhood conditions all shape health together, across both space and time.
Perhaps the more useful question is not whether upstream or downstream approaches matter more, but how interventions at different scales interact.
Small-scale interventions can sometimes build momentum for wider change. Cycling infrastructure is one example. What begins as a local scheme can gradually become part of a city-wide transport transformation once feasibility, public support and political confidence grow. Equally, broader structural policies only become meaningful through how they are experienced within neighbourhoods and communities. Housing policy, transport systems and environmental planning ultimately shape daily exposures, opportunities and stressors at local level.
Cities may therefore be uniquely important places for experimentation. They are large enough to address systemic problems, but close enough to communities for meaningful engagement and democratic participation. Some urban researchers increasingly argue that the choice between structural reform and local action is therefore a false one. Effective urban change may require interventions operating simultaneously across different scales and timescales.
I find myself increasingly persuaded by that position. Looking back, I think I once saw structural advocacy and pragmatic intervention as competing moral choices. Now I see them more as complementary forms of action. Immediate neighbourhood improvements can matter enormously to people living with disadvantage today, while longer-term structural reforms remain essential if inequalities are to narrow substantially over time.
That does not remove the tension. It probably never will. There are still difficult questions about political feasibility, displacement, gentrification and unintended consequences. Urban researchers also need humility about what evidence alone can achieve in democratic societies where people may disagree profoundly about priorities and solutions.
But perhaps the role of urban health research is not to resolve the tension between structural change and local action, but to work productively within it. Health inequalities are produced across multiple interacting systems, spaces and timescales. Our responses probably need to operate across them too.
