We have an exciting opportunity for a fully funded PhD place at the University of Glasgow. The project will join health geography / epidemiology, environmental science and cell biology. The project will be supervised by Profs Rich Mitchell, Paul Shiels and Ewan Macdonald. The funding comes from the MRC. The financial package will include a 3.5-year stipend, approved University of Glasgow fees, Research Training Support Grant (RTSG) and a conference allowance. (more…)
Author: Rich Mitchell
-
What is equigenesis and how might it help narrow health inequalities?
The health gap between more and less advantaged people persists in many countries and settings around the world, including the UK and Scotland. There is masses of research on these health inequalities. We understand that they are caused by systematic differences in access to things like a good education, good and consistent employment, reasonable income level, a safe physical environment and participation in supportive social networks. (more…)
-
CRESH research on children and the outdoors mentioned in House of Lords debate
Research by Rich Mitchell was mentioned in a House of Lords debate on 16 May. The debate centred on the contribution of outdoor activities to the United Kingdom economy and to the health and well-being of the population. The research cited was completed in 2009. Rich Mitchell and Rebecca Shaw followed a group of children (average age 13) undertaking an outdoor education scheme; the John Muir Award. The children completed questionnaires before, during and then 18 months after, their Award experience. The study showed massive inequalities in experience of outdoor environments. Children living in the poorest circumstances were over 6 times more likely to have had no prior experience of wild places than their more affluent peers. The study showed that participation in the Award increased aspirations for visiting the outdoors, particularly among the most deprived children, but it did not affect actual visiting behaviour.You can find out more about the John Muir Award hereThere is a summary of the research hereThe full report is here -
Greener urban areas in Scotland are not healthier
Studies from around the world have looked for links between how much green space a neighbourhood has and the health of the resident population. We expect to find this link because evidence from experimental studies in the laboratory and field suggests that being in natural environments may reduce stress, enable recovery from fatigue, lower blood pressure and promote healing. Green spaces may also encourage physical activity, and social contact. However, not all studies find a link between green space and health; the relationship seems to vary by country, gender, socio-economic position and, importantly, by the measure of health used.
Until recently there had been very little work looking at the relationships between green space and health in Scotland specifically. On March 11th, results of the GreenHealth programme are being launched at a conference in Edinburgh. CRESH was part of GreenHealth, together with colleagues from several other institutions in Scotland including The James Hutton Institute and our friends at the OPENspace Research Centre. In this blog I am going to tell you about some of the results from our part of the work.
A key part of our work was to look at the link between how much green space a neighbourhood has, and its rates of mortality and morbidity. The graph below is typical of the results we found.

The graph shows the relationship between the amount of green space in urban neighbourhoods in Scotland, and the risk of mortality for working age men. The risk is shown relative to urban areas with the least amount of green space, and the further a bar extends below the horizontal axis, the lower the risk in that type of area. The risk of death excludes that from external causes such as traffic accidents or suicide. The graph shows that in England and Wales, the risk of mortality falls as the amount of green space in an urban neighbourhood increases but in Scotland, there’s no significant relationship.
We spent a long time looking at whether these relationships were different for men and women, for older, working and younger age people, for more and less urban areas, for richer and poorer groups, for deaths from cardiovascular and respiratory disease, for measures of self-reported illness, and for different definitions of green space and neighbourhood. We only found a significant, protective relationship between mortality and green space for working age men living in the poorest two income-deprivation quartiles. Among these working-age men, those resident in the greenest urban areas were about 16% less likely to die than those resident in the least green urban areas.
On the whole though, we found very little evidence supporting the idea that urban neighbourhoods with more green space also have lower rates of mortality and morbidity.
The absence of effects for women echoes findings in England and Wales, and is likely linked to gender differences in the frequency and type of green space use. Women are known to use green spaces less often than men. We have written about this in the past and you can read our paper about it here.
So – why don’t we see a strong link between how much green space there is in a neighbourhood in Scotland, and how healthy it is? It seems very unlikely that the beneficial biological and psychological processes which being in green space seem to trigger, just don’t happen to Scottish people. We may be different up here, but we’re not a different species…
We checked to see if our methods, or the data sets used might explain it, but we got the same results whichever data or method we tried. We could not allow for differences in the quality or types of urban green space within Scotland, and between England, Wales and Scotland, and it is possible that this is partly responsible; perhaps urban green spaces in Scotland are smaller, or less conducive to use. Perhaps the weather is so awful up here, that people just don’t want to go outside (though, it has been known to rain in Wales too…). We also wondered whether the so-called Glasgow effect was responsible, but we got the same pattern of results when we excluded Glasgow from the analysis.
Our best bet is that the Scottish population has a higher level of underlying poor health and risky behaviours such as smoking and drinking. The impact of green space on risk of mortality is, even in England, relatively weak. Any benefits of green space in urban Scotland may just be swamped by other things that damage health.
It’s not all bad news though. Whilst greener neighbourhoods might not be healthier in urban Scotland, the people who actually visit and use green spaces, whether for exercise, or just to get away from it all for a while, do seem to have better mental health and more life satisfaction, all else being equal We have published some of those results already and blogged about them too. We have more evidence that folk who do use green spaces reap health and wellbeing benefits, and will be blogging more about it once those studies are published.
In the meantime, the message is that park down the road will probably do you an awful lot more good if you actually visit it…
-
What if neighbouring areas are very different?
Waldo Tobler’s first law of geography is that “everything is related to everything else, but near things are more related than distant things.” This is an important idea for many aspects of spatial science, but it’s taken particularly seriously by people who draw maps and do statistics to investigate how and why disease rates vary from place to place.
If Tobler’s first law holds, we should expect the characteristics of people and places who are close together (including their health) to be similar. So, in general, the folk who live in your neighbourhood should be more like you than the folk who live on the other side of town.
This matters when we are researching if and how environment affects health. We know that people’s health can be affected by a huge range of things. If we are to reveal the health impacts that environment has, we need to try and allow for as many of those other influences as possible. However, we know that it’s very hard to account for all of them. This means some of the relationship between environment and health we see in our analyses may actually be due to these ‘unmeasured’ influences, a problem we call ‘residual confounding’. Now, if Tobler’s law is right, it is also likely that these unmeasured influences are also more similar when they are closer together. When this happens, it’s called residual spatial confounding. If we don’t allow for it, we run the risk of making mistakes in assessing the strength of relationships between the characteristics of environments and the health of the people who live there.
The good news is that these problems have long been known about and there are a range of techniques to try and deal with them. They include ways to statistically ‘smooth’ maps showing how risk of a disease varies from area to area, and to adjust measurements of risk for how close together they are in geographic space.
The bad news is that Tobler’s first law is not always true! It’s not always the case that neighbouring areas do have similar characteristics or environments. Often areas that are right next to each other contain very different types of people and have a very different environment. You have probably experienced this when walking around a town or city. You cross a road, the housing changes dramatically, and the streets ‘feel’ different. Those statistical techniques assume that kind of sudden change doesn’t happen.
Dr Duncan Lee and Prof Rich Mitchell have just finished an ESRC funded research project (RES-000-22-4256) trying to improve the way we handle this situation in our research. We have successfully created, and published techniques that can spot when two neighbourhood areas are so different that we need to alter our statistical assessment of the relationships between health and environment. One technique, published in Biostatistics, can be used when we have data that tell us something about the characteristics of the people or the neighbourhoods, such as house prices or smoking rates. The other can be used when all we have is information about health in the areas (now in press with Journal of the Royal Statistical Society Series C) .
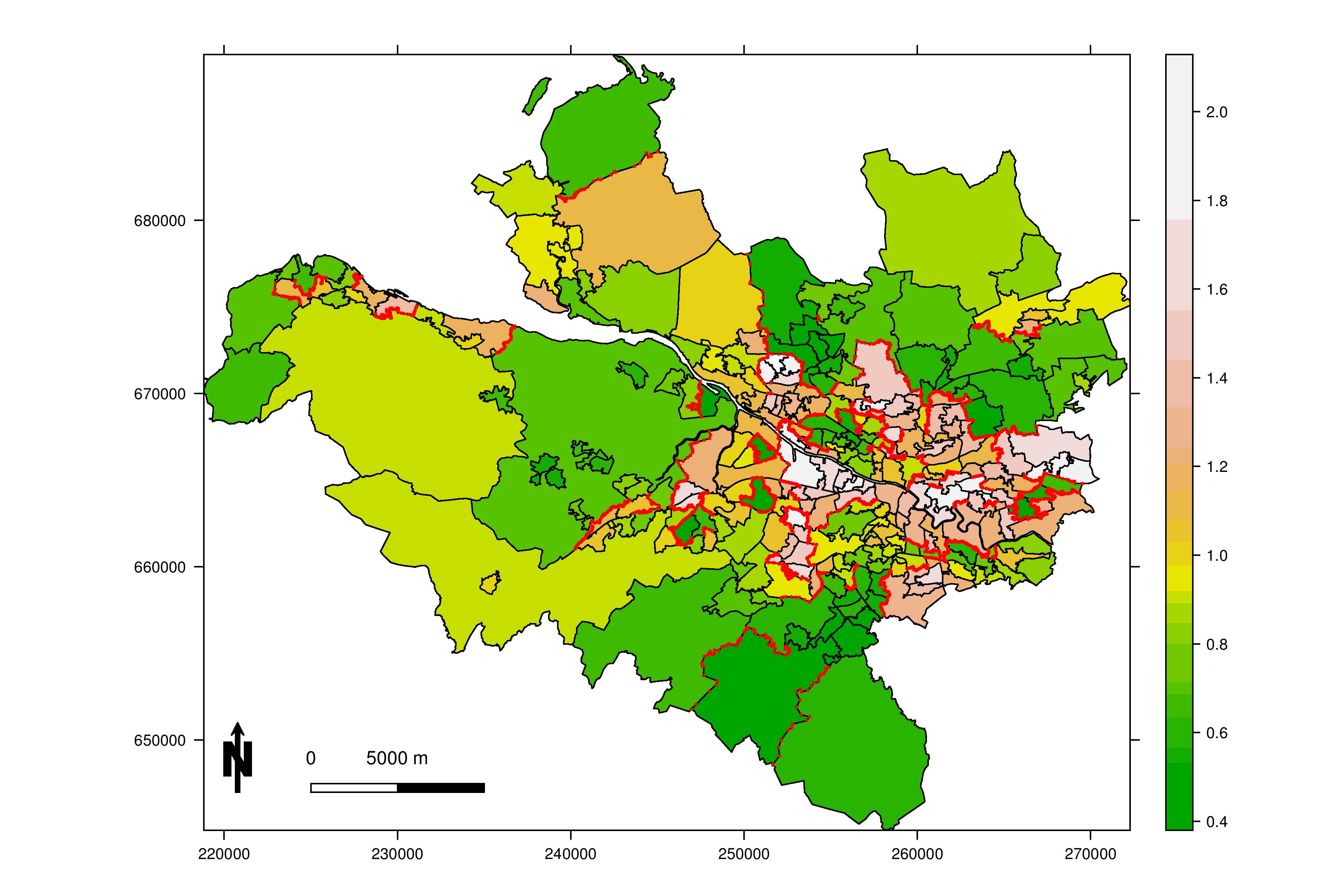
Here’s an example of our results. The map below (click it to view full size) shows 271 areas that make up the Greater Glasgow and Clyde Health Board (for the geeks, the areas are intermediate geography zones). We obtained data on the risk of admission to hospital with a primary diagnosis of respiratory disease, from the Scottish Neighbourhood Statistics database (http://www.sns.gov.uk/). The map is shaded so the colour of each area denotes its disease risk, with a value of 1.0 representing an average risk across the whole health board. Values above 1.0 represent high risk areas (for example a value of 1.10 indicates a 10% higher risk), while values below 1.0 represent low risk areas (for example a value of 0.85 indicates a 15% reduced risk). The red lines show boundaries between neighbouring areas that contain populations at very different risk of hospital admission for respiratory disease. These are the areas in which the conventional techniques would make mistakes. There are 173 of them… that’s 25% of all the boundaries in the map.

Data and boundaries © Crown Copyright. All rights reserved 2010.
We have created a free software package that will allow anyone to apply our techniques. It’s called CARBayes and is for the statistical software R. You can read about it and get it from here.
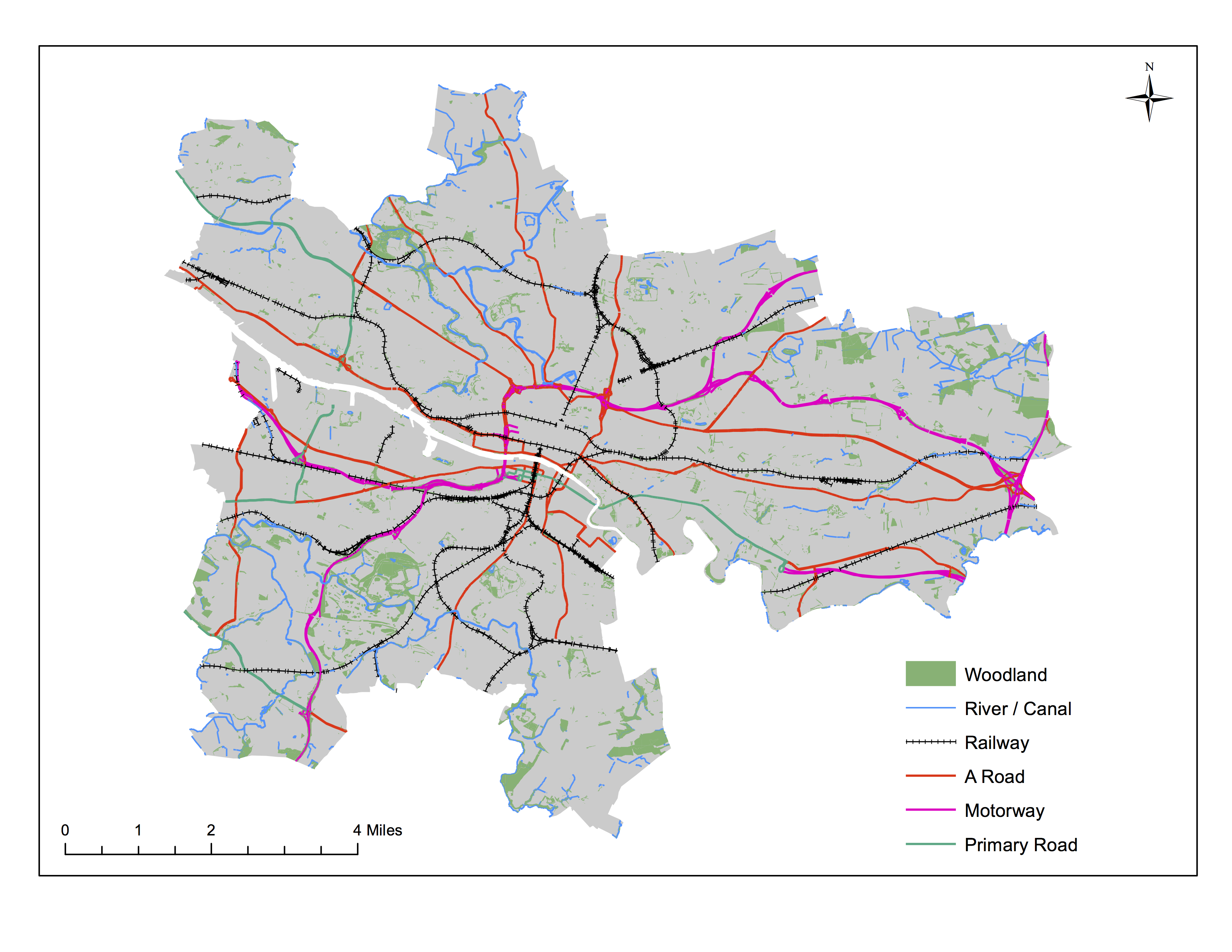
There has also been an interesting spin off from this research. Within Glasgow, we found a lot of neighbourhoods that were right next to each other but were very different in social and economic terms. We called these between-neighbourhood differences ‘social cliffs’. It prompted us to ask how such social cliffs occur. One idea is that they may be made more likely by physical barriers between the neighbourhoods, such as rivers, main roads or railways.The map below (click it to view full size) shows the kinds of physical features we’ve been looking at (note, our data are for the period before the new M74 motorway was opened).

Map based on data that are © Crown Copyright/database right 2012. An Ordnance Survey/EDINA supplied service.
Our research is now complete and we’re writing it up for publication. It seems that two kinds of physical feature are especially important. Where one or both of them lie along a neighbourhood boundary, it’s much more likely that the neighbourhoods will be very different socially, and economically. Which two do you think they are?
-
London 2012: inspiring a generation and regenerating East London?
Immediately following the Olympics, Prime Minister David Cameron announced that government funding to support Team GB athletes would increase up to the Rio 2016 Games. “The motto of these Games has been ‘Inspire a generation’. Nothing has been more inspirational than seeing our elite athletes win Gold this summer. There’s a direct link between elite success and participation in sport” he said.
This link between the inspiration of elite athletes and wider public participation in physical activity was a key claim made for the London Olympics from the start. The London 2012 Candidate file, part of the initial bid for the Games, stated that the Olympics would: “…inspire a new generation to greater sporting activity and achievement, helping to foster a healthy and active nation.”
Furthermore, the Government’s Legacy Action Plan published in 2008 promised that the Olympics would “transform the heart of East London” the home of the Olympics Park by “turning one of London’s most deprived areas into a world-class district for living, leisure, business and sport, with safe and sustainable neighbourhoods, new parkland, new homes, jobs, and social and leisure facilities for generations to come.”
So, what is the evidence regarding the impacts of large scale sporting effects on public participation in sport and area regeneration?
A review of research into the impact of mass sporting events on physical activity among the wider population by Murphy and Bauman (2007) suggested a lack of evidence for a public health benefit. A systematic review of the health and socioeconomic impacts of major multi-sport events published in 2010 by McCartney and colleagues found that few studies looked at health outcomes and concluded similarly: “The available evidence is not sufficient to confirm or refute expectations about the health or socioeconomic benefits for the host population of previous major multi-sport events.”
Sport is not the only way that London 2012 might affect health and wellbeing. Huge amounts of construction and regeneration in East London have already taken place or are planned. Yet the impacts of that are also uncertain. A review by Davies (2010) of sport and economic regeneration also highlighted that “…no comprehensive longitudinal post-event study has ever been undertaken on the economic regeneration impacts of the Olympic Games”.
The impacts of regeneration for London 2012 are being closely watched. A longitudinal study of the health and social impacts of the London Olympics upon families in East London is already underway. The Olympic Regeneration in East London (ORiEL) Study, led by Professor Steven Cummins at Queen Mary, University of London, is a five-year study, following approximately 1,800 school children and their parents in Tower Hamlets, Hackney, Newham and Barking and Dagenham. It will assess their health and well-being over time. The results of this study should demonstrate whether claims that have been confidently made for the long term public benefits of the 2012 London Olympic games, and the regeneration accompanying them, prove to be true.
-
New review shows socio-economic position over the life course affects quality of life
A new systematic review looking at the relationship between socio-economic position over the life course and quality of life has just been published in BMC Public Health by CRESH PhD student Claire Niedzwiedz, Rich Mitchell and colleagues at the University of Glasgow and MRC/CSO Social and Public Health Sciences Unit.
The review’s aim was to gather and examine evidence about how people’s quality of life as adults depends on the social and economic circumstances they have experienced throughout their life, from childhood onwards. Do childhood circumstances matter? Does it help if people move ‘up’ the socio-economic ladder? Does it harm if people move ‘down’?
In chronic disease epidemiology, several conceptual models have been developed to help explore these ideas and they provide a foundation for investigating life course effects. The accumulation model hypothesises that adverse socio-economic experiences have a cumulative, dose–response effect on health. The latent model (or critical period) suggests that circumstances during childhood have an effect on health, over and above adult circumstances. Pathway models emphasise the importance of trajectories across the life course. Social mobility models are usually divided into intra-generational and inter- generational where inter-generational mobility refers to a change in social class between generations and intra-generational mobility is the movement between different social classes in adulthood. The mobility models suggest that change in your socio-economic position will affect health, and in general lead us to expect that movement ‘up’ the social ladder is good for health, but movement down may be bad.
The review identified 12 relevant articles which used data from different five countries.
The evidence supported an overall relationship between socio-economic position over the life course and quality of life but results for each life course model were mixed. There was some evidence to suggest a latent effect of childhood socio-economic position on later quality of life for women, but the effect was not found for men. Overall, results for social mobility models suggested little effect. We found very few studies that actually assessed inter-generational mobility or accumulation and pathway effects.
There was a very wide range socio-economic position measures, outcomes, analytic techniques, reference populations and quality across all the studies we looked at. This led to a key message from the review; the need to increase study comparability. A second key message was the need for comparable data and studies from different countries. This may help to uncover aspects of different societies that influence the relationship between socio-economic position over the life course and quality of life.
You can access the article here: http://dx.doi.org/10.1186/1471-2458-12-628.
-
Key questions for researching natural environments and health
There was a long session on natural environments and health at the Royal Geographical Society /IBG conference yesterday. It was put together by Dr Liz Richardson, from CRESH, and it featured an intriguing range of 9 papers. All were exploring the relationships between natural environments and health, but there was great variety in the perspectives, methodologies and opinions on display. The session felt like a nice summary of many current issues and questions in the field.
You can read the abstracts for the papers in the first part of the session here, and the second part of the session here. At the end, I led a discussion which tried to bring together the range of questions and perspectives in the session. Here’s what we talked about.
What can we expect natural environments to do for us? Nina Morris, from Edinburgh University, used the lovely expression ‘mission creep’ in her talk and it prompted us to note that green spaces suddenly seem to be responsible for doing an awful lot. If you believed everything you read, you might think that your local park or forest will cure all ills, make everyone thin, make everyone happy, be a boon to the local economy, prevent climate change and protect rare species. It’s likely that some natural environments can contribute to some of these things, some of the time, but they’re not miracle-workers. Keeping expectations realistic and evidence-based is important.
Several talks began with the assertion that green space is thought to be, (or even known to be) ‘good for health’. There were also anecdotes that, when hearing about plans for or results from research on natural environments and health, some policy makers, journalists (and even research funders) reply “we know that already”. So, we debated, is our job done? Do we now know enough about the relationships between natural environments and health? Can we stop researching it and turn our attention to something else? Perhaps not surprisingly, a room full of researchers disagreed… I do think they had good reason though. Some of the papers really challenged what we thought we knew about whether and how natural environments are related to health. The paper from Katherine Ord, a PhD student at CRESH, for example, strongly questioned the role of physical activity in the relationship between green space and health. Whilst we’re still discovering that we know relatively little about how, when and for whom natural environments matter for human health and wellbeing, there is more work to do. The fact that many people seem now to believe that ‘green space is always good for everyone’, makes the research even more important.
Assuming that there is more work to do, what kind of research is needed? There was much talk about the value of different approaches. Qualitative, quantitative and mixed methods studies were all on display and the range of insights and types of knowledge was a powerful argument for variety in study design and methodology. The epidemiological studies CRESH specialises in are important for learning if and how natural environments contribute to the health and wellbeing of populations, and how they relate to health inequalities. But the insights from qualitative work into how and why individuals use, move within and feel about natural spaces provide crucial depth in understanding. The need to study non-natural environments as part of our research (akin to a control group) was another thread running through the debate. This is vital to be sure that any apparent impacts on health and wellbeing are a function of the natural environment itself and not something else, like just being in a different environment, or a much loved place.
Finally, we discussed the need to understand how we should manage natural environments and our access to them, to maximise their potential benefits. A paper from Michelle Newman at Coventry University, for example, took a critical look at the issues surrounding children’s access to green space in schools. Its exploration of ideas about accessing ‘risky’ environments and who is paying for (and therefore controlling) access to these spaces, prompted wider thoughts about what kinds of spaces to preserve, make accessible or construct. There is a need to ask who has access and who uses their access. Governments and policy makers now explicitly acknowledge the values of green space for health and wellbeing, which is great. Would it be so great if they started to set targets for green space use, or even compel it?
It was a fascinating, useful (and long…) session.
-
Regular physical activity in natural environments halves risk of poor mental health
Regular exercise in a natural environment may cut the risk of suffering from poor mental health by half, according to a new study published by CRESH today.
Rich Mitchell studied the use of natural and non-natural environments for physical activity, like walking, running and cycling. He found regular use of natural environments such as forests and parks seemed to protect against mental ill-health, whilst use of non-natural environments like a gym, did not.
Previous experimental studies have shown that exercise in natural environments has a positive effect on biomarkers and self-reports of stress, on mood and reported levels of fatigue. This new study was designed to look at whether such effects can be detected in the general population in every day settings.
Data from the Scottish Health Survey 2008, described the different environments in which 1890 respondents were physically active, including woodlands, parks, swimming pools, the gym, the streets and the home. The data also showed how often respondents used each environment and how physically active they were overall. Rich looked at the association between use of each environment and the risk of poor mental health as measured by the General Health Questionnaire. Only activity in natural environments was associated with a lower risk of poor mental health.
Rich said “I wasn’t surprised by the findings that exercise in natural environments is good for your mental health, but I was surprised by just how much better it is for your mental health to exercise in a green place like a forest, than in other places like the gym.”
“Woodlands and parks seemed to have the greatest effect, so the message to doctors, planners and policy makers is that these places need protecting and promoting.
“The results suggest that making the decision to exercise in a natural environment just once a week could be enough to gain a benefit. Any additional use may have a bigger effect.”
The study, published online by Social Science & Medicine, revealed that local pavements or streets was the environment most commonly used regularly for physical activity, followed by home/garden. Around 50 per cent of the sampled group reported using any natural environment at least once in the last month.
Rich did not know the type, duration or intensity of activity conducted in each environment and noted that this was a weakness in the study, but is also an area that could be looked at in more detail in future.
You can see Rich talking about the study here: http://itunes.gla.ac.uk/web/news/video/RichardMitchell.mp4
You can read the full study here http://dx.doi.org/10.1016/j.socscimed.2012.04.012 (access required). If you don’t have access and want to read it, please email Rich at Richard.Mitchell@glasgow.ac.uk and ask for a copy.
The research was funded by the Scottish Government’s Rural and Environmental Science and Analytical Services division (RESAS).
-
Are experimental studies always best?
Work has begun on our NIHR funded evaluation of Forestry Commission Scotland’s Woodlands In and Around Town (WIAT) scheme. WIAT aims to improve quality of life in towns and cities by bringing neglected woodlands into management, creating new woods and supporting people to use and enjoy their local woods. Our study, led by Catharine Ward Thompson at OpenSpace, is focused on whether changes to the local woodland environment affect people’s health. The WIAT evaluation is exciting partly because it’s a rare opportunity to ask what impact environment has on health, at a population level, via an experimental study.
The vast majority of evidence about how health and behaviour are affected by environment comes from cross-sectional studies. In cross-sectional studies, we measure both the environmental characteristic of interest (for example, how much green space there is in a neighbourhood), and the outcome of interest (for example, how healthy or happy the residents of that neighbourhood are) at the same time. Cross-sectional studies are great for suggesting links or associations between environmental characteristics and health or related behaviour, but they have many problems. In particular, we can’t be certain that the aspect of environment we are interested in causes the health outcome in question. In the case of green space and health for example, we worry that the apparent relationship between access to green space in a neighbourhood and good health among residents is really because the residents of greener neighbourhoods tend to be wealthier, and wealthier people are more likely to be healthier anyway. So, it might be that access to green space in a neighbourhood doesn’t cause better health, it’s just that healthier people are more likely to live in greener neighbourhoods.
Experimental studies are very different. In an experiment, we deliberately alter some aspect of the environment for one group of people (the intervention group), but not for another very similar group of people (the control group). We then compare what happens to health or related behaviour in the intervention and control groups. If health improves in the intervention group, but not in the control group, we can be more certain that the change in environment has caused the change in health. So, in our WIAT study, we’ll be comparing what happens to the health of communities whose woodlands are improved and promoted, with those whose woodlands are not. (That sounds a bit unfair on the ‘control’ communities but, in fact, they’ll be eligible to get their woods improved later).
A lot has been written recently about how important experimental studies are*, how much better they are for telling us ‘what works’ to improve health and behaviour, and how we need far more of them. The idea has taken hold, helped by research funding and by the fact that some key journals in public health and epidemiology now refuse to even peer review studies that are cross-sectional. Jim Dunn and Martin Bobak’s editorial* on taking over the editorship of JECH is a good indication of increased interest in experimental designs from leading journals. Mark Petticrew has also written* about it.
I am excited about the prospect of experimental studies being used to examine the impacts of environment on health and health-related behaviour. I believe that the characteristics of the places we live and work in can be a strong influence on our health and behaviour and, in turn, I think that environment could be an effective lever for improving population health and narrowing health inequalities. Experimental studies are, in theory, the best way of finding out if my ideas are right or not.
However, I do have a few concerns about the assumption that experimental approaches are always best for researching ‘what works’ to improve public health. Their strengths have been highlighted in the literature, but there has been relatively little critical thinking about them.
The processes by which environment influence our health and behaviour are complex and life long. Environment doesn’t simply determine health and behaviour; people and environments influence each other. Think about the cycling infrastructure in Copenhagen for example. The environment there enables and encourages people to cycle, so the city’s high rates of active travel are partly because of the environment. However, the environment is so conducive to active travel because the residents use it, protect it, value it and continue to improve it.
Our relationships with different aspects of environment are also formed over the whole of our lives. Catharine Ward Thompson’s work*, for example, shows that one of the strongest predictors of whether we visit woodlands as adults was whether we did so as children. That means just changing access to woodlands in the neighbourhood may not affect immediately, or at all, residents who don’t have ‘visiting the woods’ as part of their culture.
Do we know how long it will take for an environmental change to affect health and behaviour? My guess is that the time will vary by environmental characteristic and/or the health or behavioural outcome being measured. I think, in many cases, effects will be slow to materialise. Yet the reality of research, and research funding, is that it’s difficult to sustain an experiment for a long time. In turn, this might lead us, or perhaps other less critical audiences, to prioritise interventions on aspects of environment that show a quick effect, at the expense of those which may have a greater but slower effect. Worse, if brief experimental studies find no effect of environmental intervention on health, and we think experimental evidence is the best there is, it may lead to the assumption that environment does not affect health.
I worry that in the rush to use experimental designs to see ‘what works’ for public health, we have forgotten some of what we know about relationships between health and environment specifically, and about relationships between place and identity more broadly. I think experiments are very important, but I’d like to see a more critical perspective.
What do you think?
*NB links to journal articles may require institutional/personal subscription to the journal