New research from the CRESH team using data from 124,566 shopping baskets purchased in convenience stores across Scotland has found that the purchase price of tobacco is lower in more disadvantaged neighbourhoods, largely because of the higher sales of the cheapest brands in these areas.
Cigarette smoking is one of the leading causes of preventable ill-health, hospitalisations and deaths in Scotland. Approximately 19% of adults in Scotland smoke, this rises to 32% in our most deprived fifth of neighbourhoods and falls to 9% in the most affluent neighbourhoods. As Scotland moves towards a ‘Tobacco Endgame’ the Scottish Government have a target to reduce smoking prevalence to less than 5% by 2034. A recent review of smoking projections by CRUK however suggests that Scotland may miss this target by 16 years in the poorest neighbourhoods. It is important that we continue to explore all potential determinants of smoking, particularly those that drive smoking in our most deprived communities.
We know that tobacco price is one of the most important determinants of smoking behaviour and that many smokers are price sensitive. Whilst it may appear that all tobacco products are becoming increasingly expensive, research suggests that the average tobacco price in the UK has remained relatively unchanged in real terms over the past 20 years in spite of numerous tax increases. A practice, known as ‘undershifting’, has seen tobacco companies limit price increases on the cheapest brands and instead increase the price of the most expensive brands by larger margins, thus absorbing the tax increases on the cheapest cigarettes allowing them to remain cheap (Hiscock et al. 2018). As a result, the price of the lowest priced cigarette brands has remained relatively steady and the tobacco market as a whole has become increasingly stratified by price between the cheapest ‘sub value’ , ’value’, ‘mid price’ and high priced ‘premium’ brands. We wanted to understand these differentials in price a little better, so we carried out some research that was published recently in Tobacco Control. We explored whether the price paid for tobacco (both cigarettes and roll your own tobacco) was different in different types of neighbourhoods. We compared areas by deprivation, by the density of tobacco outlets and by rurality.
We analysed tobacco purchase data provided to us by The Retail Data Partnership. We looked at more than 124,000 purchases in 274 stores across Scotland in April 2018. For cigarettes the average price paid for a pack of 20 was £8.49, ranging from £7.20 to £13.25. For roll your own tobacco (RYO) 30g the average price paid was £12.14, with prices ranging from £9.80 to £15.99. We found that the price paid for tobacco did vary by neighbourhood type. In neighbourhoods with the lowest average household income the average purchase was 50p less for a pack of 20 cigarettes, and 34p less for roll your own tobacco compared with the most affluent neighbourhoods.
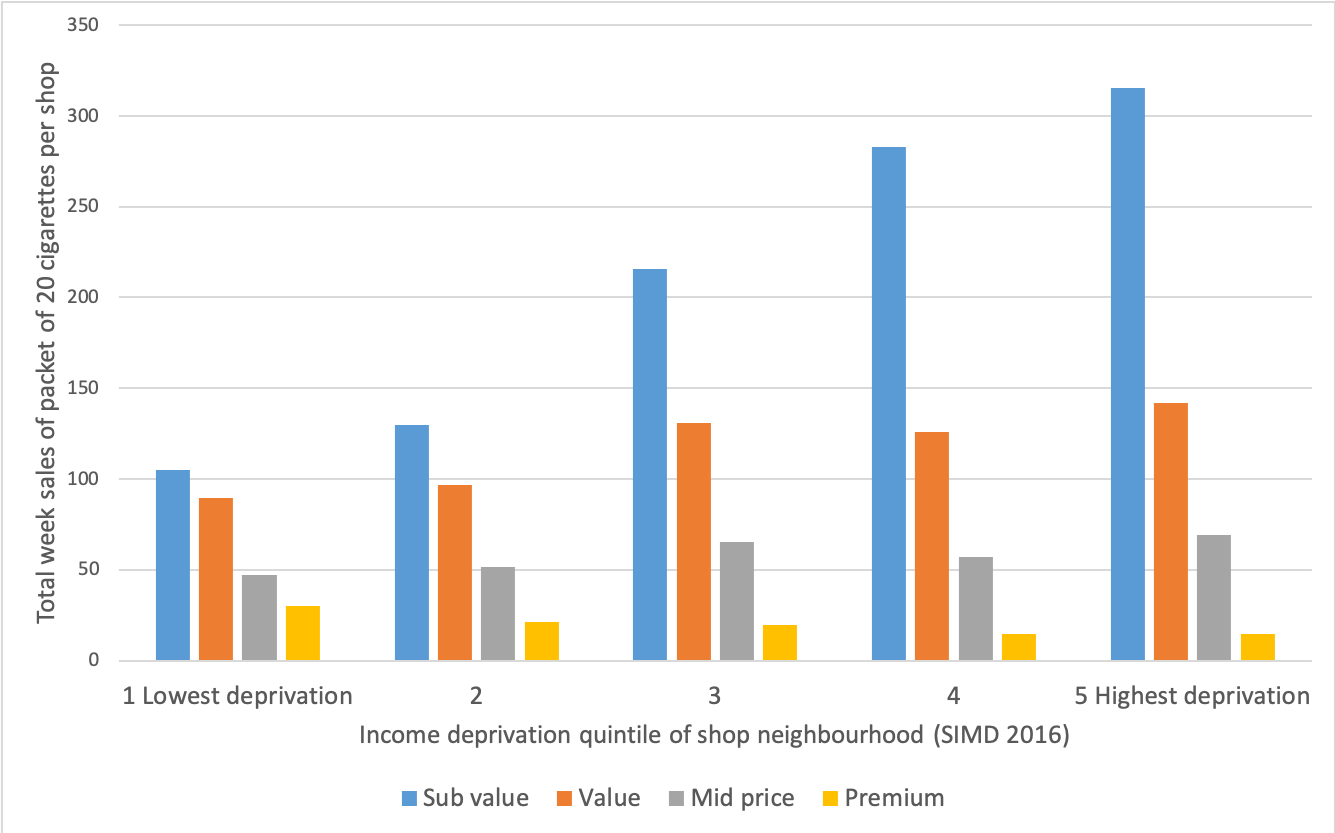
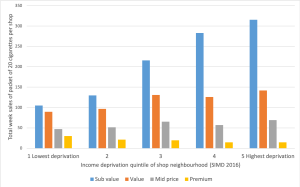
We then asked whether this was driven by individual brands being cheaper in more deprived areas, or whether cheaper, sub-value, brands were just more popular in such places. We found little evidence that individual brands were priced differently. Although the cheaper brands are the most popular in all neighbourhoods and across Scotland, accounting for 52% of sales, there’s a big difference in popularity between more and less deprived areas, In the most deprived areas these brands account for 58% of sales, but in most affluent areas it was just 39% (See Figure 1 below). So, it is the dominance of cheaper brands in more deprived areas that drives the 50p difference in average price paid per pack between deprived and affluent areas. Remember this matters because the tobacco companies work to subdue tax-based price rises on the cheapest brands.
We also explored whether the density of tobacco retailers and/or rurality had an impact on tobacco price. We found little evidence of a density effect, but we did find that the individual brands analysed were significantly cheaper in rural areas.
So what does this mean and what can we take from this research? It is clear from the CRUK review that we need to work harder in order to reach the 2034 target of less than 5% of the population smoking. Price is a lever that we can pull, but to date this has been largely done through tax increases. This research shows us that the cheapest brands are the most popular in all neighbourhood types, but much more so in our most deprived neighbourhoods where smoking rates are highest. We found that the price paid for tobacco is lower in more deprived areas compared to more affluent areas. Our results confirm that the dominance of cheaper, so called ‘sub-value’ brands in more deprived areas, is a driving force behind the difference in price paid for tobacco between neighbourhoods. This highlights the importance of cheaper tobacco products to the consumer and the market. Cheap tobacco may help tobacco companies to retain price sensitive consumers who live in the most deprived areas, which, in turn, contributes to health inequalities. In addition to increases to the duty rates on tobacco, more radical policy responses are likely to be required. These include a combination of minimum unit pricing (MUP) and a price cap at the upper end. The MUP would raise the cost of cheaper cigarettes and the price cap at the upper end would prevent the more expensive brands being used to ‘protect’ the cheaper ones from tax rises.
With growing international interest in the ‘Tobacco Endgame’, policymakers should identify measures that counter industry tactics that enable the continued sales of cheap tobacco. We published this paper in the first week of the COVID-19 pandemic in the UK. These are clearly strange times and we should rightly focus on the public health impacts of the global pandemic, and in particular the vast health inequalities that are arising. We must not however forget that the public health challenges we were faced with before this pandemic remain. Tobacco, and other unhealthy commodities, require our attention and the inequalities that arise from them remain a matter of social justice.
You can find the paper here:
Shortt, N., Tunstall, H., Mitchell, R., Coombes, E., Jones, A., Reid, G. & Pearce, J. Using point-of-sale data to examine tobacco pricing across neighbourhoods in Scotland. Tobacco Control, Published Online First: 19 March 2020. doi: 10.1136/tobaccocontro
References
Hiscock R, Branston JR, McNeill A, et al. Tobacco industry strategies undermine government tax policy: evidence from commercial data. Tob Control 2018;27:488 LP – 497. doi:10.1136/tobaccocontrol-2017-053891